視頻報道
-

椎管內囊腫病例:藏在脊柱中的惡魔
CCTV-4《中華醫(yī)藥》
-
突出的腫瘤-腦膜瘤
CCTV10《走進科學》
相關文章
IDH-1R 1 3 2 Hmutation status in diffuse glioma patients:implications for classification
2018-07-17 11:26 作者:三博腦科醫(yī)院
王鵬斐 劉寧 宋洪旺 姚坤 江濤 李守巍 閆長祥
首都醫(yī)科大學三博腦科醫(yī)院 北京市神經外科研究所
Abstract:
WHO2007 grading of diffuse gliomas in adults is well-established. However, IDH mutations make classification of gliomas according to the WHO2007 edition controversial. Here, we characterized IDH-1R132H mut status in a cohort of 670 adult patients with different WHO2007 grades of diffuse glioma. Patient characteristics, clinical data and prognoses were obtained from medical records. Patients with IDH-1R132H mut were younger and had better clinical outcomes than those without mutations. Differences in age among patients with astrocytomas of different WHO2007 grades were eliminated after patients were grouped based on IDH-1R132H status. IDH-1R132H mut was present more often in patients with lower Ki-67 and MGMT protein levels and higher mutant p53 levels. Ki-67 was also strongly associated with WHO2007 grade independently of IDH-1R132H mut status. Moreover, patients with Ki-67≥30 survived longer than those with Ki-67<30, regardless of IDH-1R132H mut status. Patients in the IDH-1R132H mut group with lower MGMT protein levels also had better clinical outcomes than those in other groups. Our results indicate that to better treat gliomas, IDH mutation status should be included when determining WHO2007 grade in glioma patients.
Introduction:
Gliomas are the most common primary brain tumors, accounting for 31% of all central nervous system tumors and 81% of malignant CNS tumors [1], and are classified into grades from I to IV on the basis of histopathological and clinical criteria established by the World Health Organization (WHO) [2]. Grade I gliomas are often circumscribed and generally curable with surgical resection alone [1, 2]. In contrast, Grade II and III gliomas are invasive and progress to higher grade lesions, with a poor prognosis [1, 2]. Glioblastomas, which are WHO grade IV gliomas, are traditionally classified as either primary or secondary if they developed from lower-grade gliomas [2]. Analyzing the specific genetic characteristics of gliomas has improved the understanding of glioma genesis and predictions of prognosis, and allows for the use of targeted treatments on an individual basis [3, 4]. IDH (Isocitrate Dehydrogenase) mutations are among the most common gene alterations in gliomas. Mutations in IDH genes occur in up to 80% of astrocytomas, oligodendrogliomas, oligoastrocytomas, and secondary glioblastomas, and in less than 10% of primary glioblastomas [5, 6], indicating that this mutation plays a key role in early gliomatogenesis [7]. Patients with grade II, III, or IV gliomas carrying IDH mutations have better overall survival [4, 8]. Additionally, accounting for IDH mutation status eliminates age differences in the prevalence of different WHO2007 grade gliomas [9, 10]. These results indicate that additional characteristics in addition to WHO2007 grade should be considered when classifying gliomas.
Studies of IDH-1 mutations are frequently based on DNA sequencing, a method which is usually considered robust. However, the IDH1 R132H antibody (clone H09) is more convenient, reliable, and consistent for the detection of IDH1R132H protein, and is widely used in clinical diagnosis and research [11-15]. In this study, in addition to IDH-1R132H mut protein levels, Ki-67 index and mutant P53 and MGMT (O (6)-methylguanineDNA methyltransferase) protein levels were explored in a cohort of glioma patients from a single institution in China. The predictive value of IDH-1R132H mut levels for glioma patient prognosis was also investigated in this study.
Results
1. IDH-1 R132H mutations in various histological types
We analyzed the distribution of IDH1R132H mut in 33 astrocytomas (A), 41 oligodendrogliomas (O), and 84 oligoastrocytomas (OA). The IDH1R132H mutation was present less often in A, at 60.6%, than in O or OA (both 84.1%, p=0.006) (Table 1). We also investigated the presence of IDH1R132H mut in 126 anaplastic gliomas, including 32 anaplastic astrocytomas, 39 anaplastic oligodendrogliomas, and 55 anaplastic oligoastrocytomas. The distribution of IDH-1 mutation did not differ among the anaplastic glioma subtypes (Table 1). There were 300 primary glioblastomas (pGBM), 62 secondary glioblastomas (sGBM), and 26 glioblastomas with an oligodendroglioma component (GBMO). The rate of IDH-1R132H mut was 6.3% in pGBM, lower than that in sGBM (71.0%, p<0.001) and GBMO (46.2%, p<0.001). IDH-1R132H mut was also more frequent in sGBM than in GBMO (p<0.05) (Table 1).
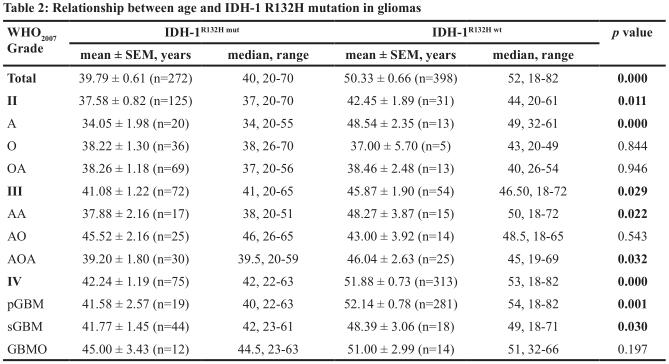
2. IDH1 R132H mutations and age
The 272 patients carrying IDH-1 R132H mut were younger than the 398 patients without the mutation (39.79 ± 0.61 vs. 50.33 ± 0.66 years, p<0.001) (Table 2). The association between IDH-1R132H mutation and younger age in astrocytic tumors contributed to this difference (Table 2). Furthermore, we analyzed age differences in patients with astrocytic neoplasms. Patients with pGBM (51.47 ± 0.76, n=300) were older than those with AA (42.75 ± 2.30, n=32; p=0.001) or A (39.76 ± 1.95, n=33; p<0.001). Patients with AA also tended to be older than those with A, but this difference did not reach statistical significance. There were no differences in age among patients with A, AA, or pGBM in either the IDH-1R132H-wt (p=0.347) or IDH-1R132H-mut (p=0.062) groups.
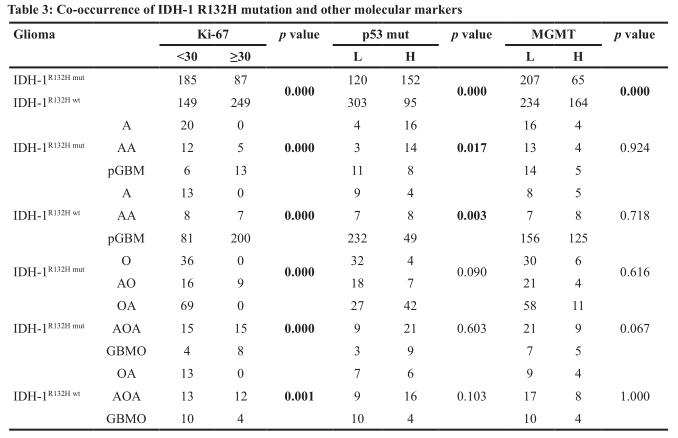
3. IDH-1 R132H mutation and other molecular markers
As shown in Table 3, 68.0% (185/272) and 32.0% (87/272) of the IDH-1 R132H-mut and IDH-1 R132H-wt groups, respectively, had Ki-67<30. A, O, and OA patients with lower WHO grades also tended to have Ki-67<30, independent of IDH status. Mutant p53 was more prevalent in the IDH-1 R132H mut group (55.9%, 152/272) than in the IDH-1 R132H wt group (23.9%, 95/398). However, mutant p53 was only present in grade II-III astrocytomas. Increased MGMT protein levels were observed more often in IDH-1 R132H-mut patients than in IDH-1 R132H-wt patients (76.1% vs. 58.8%, p<0.001). However, there was no consistent relationship between MGMT proteins level and IDH-1R132H status within any of the individual glioma subtypes (Table 3).
4. IDH-1 R132H mutation and prognosis
Follow-up data was available for 165 pGBM, 50 sGBM, 22 GBMO, 14 AA, 28 AO, 47 AOA, 13OA, 30 O, and 2 A patients. In multivariate analysis, we found that increased IDH-1R132H mut , low MGMT levels, and Ki-67<30 were associated with better prognosis.
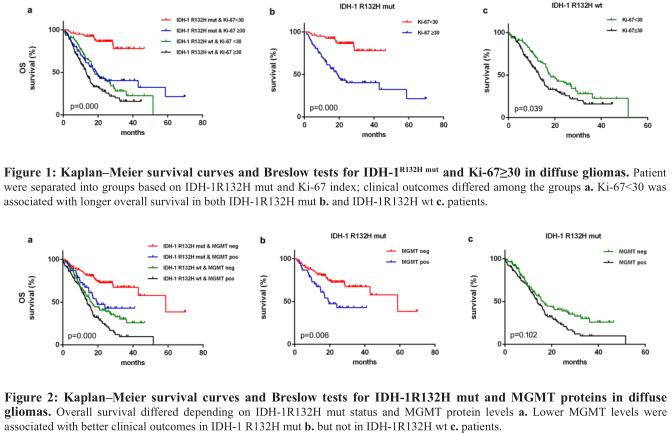
IDH-1R132H mutation and Ki-67<30: IDH-1R132H mutation was associated with better prognosis [median 58.700 months (95% CI 23.946–93.454) vs. 15.370 months in wild-type patients (95% CI 13.190–17.550); p<0.001, Breslow test]. The median OS of 36.230 months (95% CI 31.103–41.357) in patients with Ki-67<30 was higher than the OS of 15.370 months (95% CI 12.842–17.898) in patients with Ki-67≥30 (p<0.001, Kaplan-Meier method and Breslow test). We subdivided IDH-1R132H mut or IDH-1R132H wt gliomas based on Ki-67<30, and found differences in mOS among the four groups (Fig. 2a). Patients with Ki-67<30 had better prognoses, regardless of whether they had IDH-1R132H-mut [(median not reached) vs. 19.000 months (95% CI 13.754–24.246); p<0.001, Breslow test, Fig. 2b] or IDH-1R132H wt [median 17.400 months (95% CI 13.627–21.173) vs. 13.270 months (95% CI 11.141–15.399); p=0.039, Breslow test, Fig. 2c]. However, OS did not differ between IDH-1R132H mut/Ki-67≥30 and IDH-1R132H wt /Ki-67<30 patients (p=0.751, Breslow test).

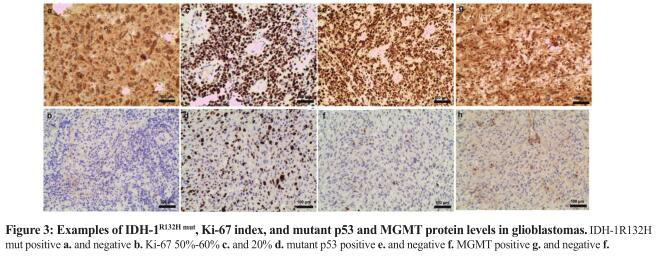
IDH-1R132H mutation and MGMT: The mOS of 15.670 months (95% CI 13.273–18.067) in MGMT-positive patients was shorter than the mOS of 32.500 months (95% CI 22.439–42.561) observed in MGMT-negative patients (p<0.001, Breslow test). Furthermore, mOS differed among IDH-1R132H-mut-MGMTneg (58.700 months, 95% CI 31.437–85.963), IDH-1R132H mut-MGMTpos (19.570 months, 95% CI 11.018-28.122), IDH-1R132H wt-MGMTneg (16.300 months, 95% CI 13.188–19.412) and IDH-1R132H-WT-MGMTpos (13.830 months, 95% CI 11.019-16.641) patients (p<0.001, Breslow test, Fig. 3a). MGMTneg patients in the IDH-1R132H mut group (p=0.006, Breslow test, Fig. 3b), but not in the IDH-1R132H wt group (p=0.102, Breslow test, Fig. 3c), had a much better prognosis than MGMTpos patients. No difference was observed in OS between IDH-1R132H-mut-MGMTpos and IDH-1R132H-WT-MGMTneg patients (p=0.471, Breslow test).
Discussion
The most frequent IDH-1 mutation type in glioma is R132H, which accounts for 88.2%-92.7% of mutations in this gene [16-18]. In an IHC study specifically detecting IDH-1 R132H mut using the H09 antibody, the rates were 83.0% in A II, 90.0% in O II, 100% OA II, 81.0% in A III, 88.0% in O III, 87.5% in OA III, 4% in glioblastoma, and 71.4% in sGBM [14]. The frequency of IDH-1 mutations ranged from 4-7.6% in primary glioblastoma and 73-88% in secondary glioblastoma [19, 20]. The IDH-1 R132H mutation rates detected here are similar to the ranges published previously [14, 17, 19, 21].
Also in agreement with previous findings, patients harboring IDH-1R132H mut in all grades of glioma in our study were younger than those without the mutation [6, 17, 22, 23]. Moreover, IDH-1R132H mut was present much more frequently in younger A, AA, AOA, pGBM, and sGBM patients. Others studies suggest a strong association between age and the prevalence of all WHO2007 glioma subtypes [6, 17]. In this regard, the differences between our findings and previous studies were likely due, at least in part, to small numbers of patients with particular gliomas subtypes examined here. A II IDHmut and A III IDHmut patients did not differ in age in a previous study [9]. While patients with A III were older than those with A II in our study, both groups were significantly younger than those with pGBM. However, there were no differences in patient age after they were separated based on IDH-1R132H mut. Thus, the differences in age associated with different WHO2007 grades may be strongly influenced by IDH-1R132H mut status.
Previous studies suggested a strong correlation between IDH mutations and lower Ki-67 index, mutant p53 levels, and MGMT promoter methylation in gliomas [10, 16, 19, 24-26]. Here, we found that lower Ki-67 was associated with IDH R132H mut in all WHO2007 glioma subtypes. However, mutant p53 expression in astrocytic tumors only differed after patients were grouped based on IDH-1 R132H mutation status. It is well-established that IDH mutations are associated with MGMT promoter methylation [10, 26-28]. In the present study, an association between IDH-1 R132H mut and MGMT protein levels was observed in glioma overall, but not within the glioma subtypes. These differences may be due to differences in the sensitivity of the detection methods [26, 29]. However, our results indicate that combining IDH-1R132H status with Ki-67 index and mutant p53 and MGMT protein levels could improve prognosis predictions in glioma patients.
Recent data suggest that IDH-1 mutations, Ki-67 index, and MGMT protein levels are prognostic factors for diffuse gliomas [15, 20, 22, 24, 30-32]. Cai et al. found that IDH-wt plus Ki-67-low and IDH-wt plus Ki-67-high astrocytic tumor patients had different clinical outcomes. The cutoff for Ki-67 in their study was 10%, and median survival was about 2 years in Ki-67-low and 1 year Ki-67-high patients [32]. Zeng et al. observed that Ki-67≥30 was associated with worse prognosis in both IDH mut (median OS=566 days) and IDH wt (median OS=355 days) groups. The median OS in our study was closer to that found by Zeng et al. These results indicate that Ki-67 index is a reliable candidate for determining prognosis in glioma patients in addition to IDH-1 status. Although the prognostic value of MGMT protein levels is controversial [29], we found here that they were predictive of prognosis. Different IHC detection thresholds may help explain this discrepancy.
In summary, we characterized the expression of IDH-1R132H mut in a large cohort of glioma patients. IDH-1R132H mut was associated with specific WHO2007 histological grades and younger age. Age differences between different WHO2007 grades of astrocytoma were strongly influenced by IDH-1R132H mutation status. Low Ki-67 index values occurred much more often in patients with lower WHO2007 grades and IDH-1R132H mutation. Finally, our study indicated that Ki-67 index and MGMT protein levels, together with IDH mutation status, were predictive of prognosis in different glioma subtypes.
Methods
Patients and tumor samples
Tumor samples were obtained from Sanbo Brain Hospital. Informed consent was obtained from all patients prior to the study. All experiments using human tissues were approved by the Institutional Review Board of Sanbo Brain Hospital. 670 adult patients with diffuse supratentorial gliomas were involved in the study. WHO classification of all specimens was performed by two independent neuropathologists [2]. In the case of a discrepancy, the two observers simultaneously reviewed the slides until a consensus was achieved. Clinical data, including patients’ age at diagnosis, sex, and molecular pathology, were collected. The diagnosis of GBMO (glioblastoma with an oligodendroglioma component) was made as previously described [33]. OS (overall survival) was measured from the date of operation to the death or the last known follow-up.
Evaluation of IDH-1R132H mut, MGMT, mutant P53, and Ki-67 levels by immunohistochemistry
Experimental procedures were performed as described previously [34-36]. Primary antibodies against IDH1R132H (Dianova 1:100), p53 (1:100 Invitrogen), MGMT (1:150 Invitrogen), and Ki-67 (1:200 Invitrogen) were used. The cutoff values were 10% for IDH-1R132H mut, 10% for mutant p53, 10% for MGMT, and 30% for Ki-67. Representative images of high and low IDH-1R132H mut (Fig. 1a, b), Ki-67 (Fig. 1c, d), mutant p53 (Fig. 1e, f), and MGMT protein (Fig. 1g, h) levels in glioblastoma patients are shown.
Statistics
SPSS 22.0 was used for all statistical analyses. The χ2 test was applied to assess the co-occurrence of IDH-1 mutation patient characteristics or the presence of other disease biomarkers. Survival curves were analyzed by the Kaplan-Meier method and the Breslow test. A p<0.05 (two-sided) was considered statistically significant.
Funding
This work was supported by grants from the National Youth Science Fund from China (No.81302200) and Key Projects in the National Science & Technology Pillar Program during the Twelfth Five-year Plan Period (No.2014BAI04B01) from China.
Conflict of interest
The authors declare that they have no conflict of interest.
(參考文獻略)
 京公網安備 11010802035500號
京公網安備 11010802035500號