視頻報道
-

椎管內(nèi)囊腫病例:藏在脊柱中的惡魔
CCTV-4《中華醫(yī)藥》
-
突出的腫瘤-腦膜瘤
CCTV10《走進(jìn)科學(xué)》
相關(guān)文章
Anatomic study of the anterior skull base via an endoscopic transnasal approach
2017-01-19 13:16 作者:王醫(yī)生
1. Introduction
Many lesions in the anterior skull base are approached through transcranial procedures in a conventional manner.The development of endoscopic techniques in skull base surgery offers new ways of dealing with the pathology of the anterior skull base. The endoscopic transnasal procedure for removal of neoplasms in the anterior skull base has achieved good outcomes and fewer complications. This paper systematically describes the anatomy of the anterior skull base through the endoscopic transnasal approach in order to provide a clinical reference.
2. Materials and methods
2.1. Materials
Thirty complete skull-base specimens (from Beijing Neurosurgical Institute) were obtained. A type-104 digital vernier calliper with 0.01-mm accuracy (United Precision Machine, Inc., Shenzhen, China) and a compass were used for the measurement of anatomic relationships. Ten Chinese adult heads (10 sides, from Beijing Neurosurgical Institute) fixed with 10% formalin solution were obtained, and the arteries and veins were injected separately with red and blue latex. Endoscopes (4- mm diameter and 0? and 30? visual field; manufactured by Rudolf Limited Corporation, Tuttlingen, Germany) equipped with a microdrill and several endoscopic surgical instruments were used.
2.2. Methods
2.2.1. Measurement of skull base specimens On skull base specimens, the distance between the bilateral optic canals was measured (between inner ridges of bilateral optic foramen). The structures of the optic canals, ethmoid plate, planum sphenoidale, anterior ethmoid foramen, posterior ethmoid foramen, and optic canal opening were revealed in an orderly manner.
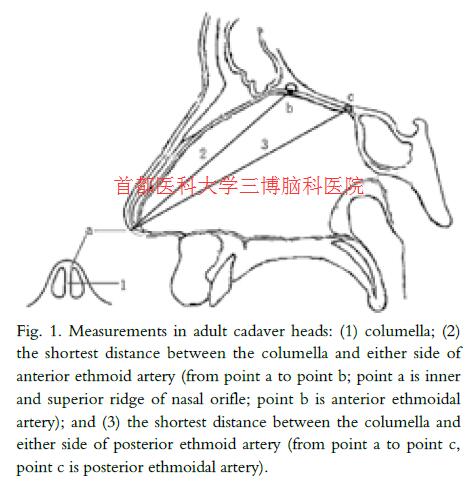
2.2.2. Dissection and measurement in fixed heads The endoscopic transnasal approach to the anterior skull base was simulated to reveal the area exposed in real operations. The distance between the columella and anterior ethmoid artery or posterior ethmoid artery was measured on both sides (Fig. 1).
3. Results
3.1. Important anatomic landmarks of the anterior skull base and endoscopically measured distances between these landmarks
3.1.1. Anterior ethmoid artery and posterior ethmoid artery
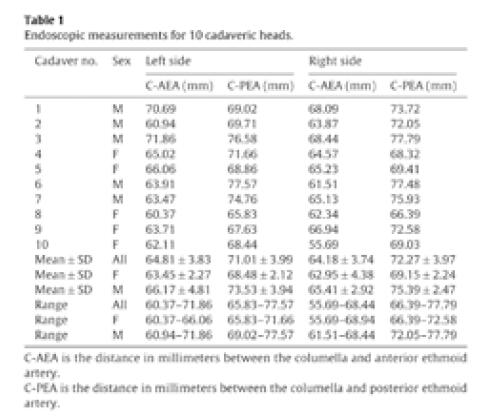
Both the anterior and posterior ethmoid arteries originated from the optic artery within the orbit and accompanied the corresponding nerves, which passed between the superior oblique muscle and medial rectus muscle. The anterior ethmoid artery was larger. Subsequently,the arteries passed through the anterior ethmoid foramen and posterior ethmoid foramen, respectively, before finally entering the ethmoid sinus. In the ethmoid sinus, the anterior ethmoid arteries passed almost horizontally through the bony canals to the skull near the crista galli and the anterior border of the ethmoid plate; they then entered the space between the two layers of the dura mater to form the anterior falx artery.The posterior ethmoid arteries reached the lateral border of the ethmoid plate and passed through the bony canals, then traveled behind the posterior border of the ethmoid plate at the front of the optic canals before entering the skull base.Themeandistance from the columella to the anterior ethmoid artery was 64.81±3.83mmfor both sexes (range from 60.37 to 71.86mm) on the left side, 63.45±2.27mm (range from 60.37 to 66.06mm) in females and 66.17±4.81mm (range from 60.94 to 71.86mm) in males. The average distance overall was 64.18±3.74mm (range from 55.69 to 68.44mm) on the right side, 62.95±4.38mm (range from 55.69 to 68.94mm) infemales and 65.41±2.92mm(range from 61.51 to 68.44mm) in males. The mean distance from the columella to the posterior ethmoid artery was 71.01±3.99mm (range from 65.83 to 77.57mm) on the left side, 68.48±2.12mm (range from 65.83 to 71.66mm) in females and 73.53±3.94mm (range from 69.02 to 77.57mm) in males. On the right side, the average distance was 72.27±3.97mm (range from 66.39mm to 77.79 mm), 69.15±2.24mm (range from 66.39 to 72.58mm) in females and 75.39±2.47mm(range from 72.05 to 77.79mm) in males (Table 1).
3.1.2. Roof of ethmoid sinus
The roof of the ethmoid sinus was inside the frontal orbital plate,which usually sloped downward (front to back) at an angle of 15?.Above the ethmoid sinus was the anterior skull fossa, and the anterior boundary was the anterior ethmoid artery; the inside of the ethmoid sinus was perpendicular to the plate of the ethmoid bone,and the orbit roof was external to the ethmoid sinus. The frontal recess (the channel for frontal sinus drainage) was bounded on the inside by the frontal and upper extremity of the middle turbinate,on the outside by the papyraceous lamina, and posteriorly by the anterior ethmoid artery. The anterior ethmoid artery separated the frontal recess (anteriorly) from the ethmoid roof (posteriorly).
3.1.3. Planum sphenoidale
The planum sphenoidale was located in the middle part of the lesser sphenoid wing. Its anterior border was connected to the ethmoid plate and the fronto-ethmoid suture. Its posterior border was at the chiasmatic groove and passed anteriorly to the clinoid process bilaterally. The two structures above formed the roof of the optic canals.
3.1.4. Optic canals
The optic canals were located inside the lesser sphenoid wing,between the sphenoid sinus or ethmoid sinus medially and the optic strut laterally. The optic nerves and ophthalmic arteries passed through the optic foramina. The mean distance between the bilateral optic canals was 15.13±1.69mm (range from 11.62mm to 17.82 mm),13.82±1.28mm (range from 11.62 to 16.37mm) in females and 16.44±0.79mm (range from 15.20 to 17.82mm) in males (Table2).

3.2. Anatomy of skull base through the endoscopic transnasal approach
3.2.1. Nasal stage
The endoscope was passed along the middle turbinate to the sphenoethmoid recess, and the sphenoid ostium between the superior turbinate, and the nasal septum was identified. The nasal septum mucosal membrane was resected from the sphenoid ostium and then dissected to expose the bony sphenoid ostium and nasal septum.
3.2.2. Sphenoid sinus and posterior ethmoid sinus
The bony sphenoid ostium was extended by removing parts of the bony nasal septum and parts of the anterior wall of the sphenoid sinus. The posterior ethmoid sinus, bilateral ethmoid plates,and perpendicular plates were resected.Mucosa was removed to locate the anterior and posterior ethmoid arteries. The sellar floor,optic prominence, carotid prominence, and bilateral carotico-optic recesses were observed and identified endoscopically.
3.2.3. Mucosal and bony layer of anterior skull base
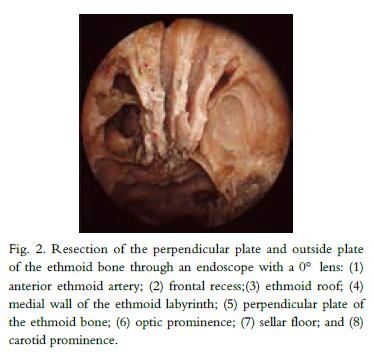
Before the mucosa was detached, some important structures in the anterior skull base such as the medial wall of the ethmoid labyrinth, perpendicular plates of the ethmoid, and anterior and posterior ethmoid arteries were identified (Fig. 2). Mucosa was removed to follow the crista galli forward, the optic canals, the orbit wall laterally, and the sellar floor backward. Bones of the anterior skull base including the crista galli, ethmoid plate, planum sphenoidale, and tuberculum sellae were drilled and the bilateral anterior ethmoid arteries and posterior ethmoid arteries were cut off. The optic prominence, sellar floor, crista galli, anterior ethmoid artery, and posterior ethmoid artery were important anatomic landmarks of the anterior skull base. The dura mater and anterior intercavernous sinus were exposed. The dura mater was dissected along the midline backward to the anterior border of the sellar floor.
3.2.4. Subdural layer of anterior skull base
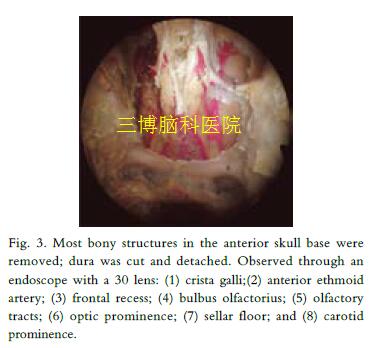
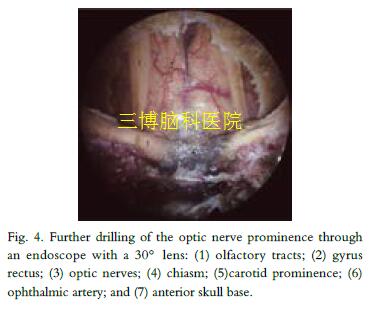
The dura mater was dissected to expose the optic nerves, the chiasm, the bilateral olfactory bulbs and tracts, and the frontal cortex (Fig. 3). The exposed area was extended forward to the bulbus olfactorius and crista galli, laterally to the rim of the olfactory tracts,and backward to the optic nerves and the chiasm (Fig. 4).
4. Discussion
Combining experience with pituitary adenoma resection through endoscopic transnasal approach with that of transnasal endoscopic repair for cerebrospinal fluid rhinorrhea,some surgeons began to treat anterior skull base pathologies through the transnasal approach. Repair of cerebrospinal fluid rhinorrhea through the endoscopic transnasal approach requires extensive exposure of the anterior skull base to identify the fistula through a narrow surgical corridor. Most structures in the nasal cavity are protected; the procedure is considered to be less invasive to normal structures in the surgical corridor than microscope surgery.Someskull-base tumors, such as meningiomas originating in the tuberculum sellae or olfactory groove, can be resected completely through this approach. Therefore,understanding the anatomy of the anterior skull base through the endoscopic transnasal approach can facilitate endoscopic surgery of the anterior skull base as well as reduce the occurrence of complications.
After penetrating the wall of the sphenoid sinus, it is necessary to resect the posterior ethmoid sinus to further expose the anterior skull base. Anatomic landmarks have to be identified to locate tumors in the anterior skull base. The anterior ethmoid artery is a common landmark for describing the position of the ethmoid roof,frontal recess, and crista galli, as well as the connection between the posterior wall of the frontal recess and the ethmoid roof.Mucosa is removed to avoid damage to peripheral structures and to identify the sellar floor and its bilateral optic prominence and surroundings. The posterior ethmoid artery is located before the optic prominence, surface of the cribiform plate, and perpendicular plate of the ethmoid bone. The anterior ethmoid artery can be located by tracing forward along the posterior ethmoid artery.Owing to the angle of the papyraceous lamina, resection of the middle turbinate and medial plate of the ethmoid sinus is sometimes necessary to expose the anterior ethmoid artery. Additionally, the anterior ethmoid artery is behind the frontal recess, and the crista galli is identified as the thick bone along the frontal midline.
The anterior and posterior ethmoid arteries are important surgical landmarks used for calculating the distance to the columella.Moreover, these landmarks also help describe the position of the above structures. Lee et al. [8] found that the average distance from the midpoint of the anterior ethmoid artery to the inside border of the columella is 63mm on the left side and 64mm on the right side (for 28 cadaver heads). Our results were similar to those of Lee et al. for both sexes, which may be because patients were of the sameace.
The area in the anterior skull base that needs to be removed depending on the pathology and extension of the lesion, as well as the function of the nasal cavity. The bone behind the anterior ethmoid artery is drilled only if olfactory nerve preservation is necessary. The posterior part of the planum sphenoidale and optic prominence are retained if the optic nerves are not involved. The distance between the openings of the optic canals inside the skull was 17±3mm(range, 13–21mm)when determined by Jho and Ha, a value that is 2mm wider than the distance observed in our specimens (15.13±1.69mm, range from 12.37mm to 17.82 mm).This differencemayderive from the racial background of the patient population. This width should be limited to 10mmif the bone of the posterior planum sphenoidale is drilled. The dura mater should be dissected along the midline and the anterior intercavernous sinus can be damaged by backward dissection. The bilateral olfactory tracts should be protected when the dura mater is cut laterally.
These results have demonstrated that endoscopic transnasal approach is feasible to expose the area from the crista galli to the posterior border of the planum sphenoidale, as found by other authors. The anatomic data as well as established anatomic landmarks associated with endoscopic surgery would benefit future clinical work. In the literature, some authors have used this technique successfully for the treatment of cerebrospinal fluid rhinorrhea, removal of encephalomeningocele, and resection of tuberculum sellae, planum sphenoidale, and olfactory groove meningiomas. Additional clinical trials will be necessary to further explore pathologies of the anterior skull base.
(參考文獻(xiàn)略)
 京公網(wǎng)安備 11010802035500號
京公網(wǎng)安備 11010802035500號